Hello Julia!
If you are sure that a small particle of an object broke off during masturbation, and not earlier, and remained in the genital tract, you should make every effort to remove the foreign body.
It is impossible to predict how a foreign body will behave in your body. Once in the vagina, a piece of plastic may for a long time not cause any disorders or pathological symptoms, can come out with natural secretions, or, conversely, go deep into the uterus and further, with the most unpleasant consequences for health.
In some cases, you can remove a foreign object from the vagina yourself using your fingers, irrigation, or forceps. But this is only if the foreign body is shallow in the vagina and is determined by palpation. It all depends on where the foreign body initially entered, whether it caused damage to the epithelium and mucous surfaces, as well as on the size and shape of the foreign body.
IN difficult cases Specialist assistance may be required to remove the item and prevent infections.
The entry of foreign objects into the genital tract is dangerous due to the possibility of developing bacterial infections, inflammation, and changes in the natural microflora.
The presence of a foreign body in the vagina can be manifested by symptoms of vulvovaginitis - leucorrhoea, hyperemia of the vestibule, burning, bloody discharge.
Carefully observe your condition and the nature of your discharge. You should be wary of discharge from unpleasant smell or unusual color. Sometimes the presence of a foreign body can cause vaginal bleeding. In this case, you should immediately consult a doctor.
If a foreign body remains in the vagina for a long time, erosion may develop. Sharp objects can lead to tissue perforation and secondary infection.
Diagnosis of a foreign body depends on the length of time the object is in the vagina, and includes a gynecological examination, colposcopy, vaginal probing, and smear examination.
If a foreign body is suspected of migrating from the vagina, the doctor may use a CT scan, scanogram, or abdominal x-ray to make a diagnosis. Ultrasound echography may also be needed to determine the location of a foreign body in the vagina and pelvis.
Treatment consists of removing the detected object using a finger, irrigation, instruments, or surgery.
The simplest and effective method removal of a foreign body - removal with urethral forceps or tweezers after visualization using mirrors.
All symptoms of infection, pain and discharge usually resolve quickly after the foreign body is removed.
In case of prolonged presence of foreign objects in the genital tract and the formation of an infection, antibiotics may be prescribed.
Most serious complications occur when infection penetrates into the deep pelvic tissues or peritoneal cavity.
Therefore, it is better not to risk your health and seek the help of a gynecologist.
Objects in the uterus are foreign bodies in the cavity or wall of the uterus, accompanied by pathological changes. Moreover, they can be quite serious, causing diseases of the female genital area: endometriosis, secondary infertility etc.
Where do foreign objects come from in the uterus?
Objects that enter the female reproductive organs are, as a rule, contraceptives: bone remains of the fetus after an abortion, surgical instruments. Intrauterine device as a primary contraceptive, it is the most commonly ingested item. It is especially dangerous that a foreign body may not manifest itself in any way for a long time, that is, it may become encapsulated. Naturally, an inflammatory process begins in the female body, which cannot be actively treated and can last for years.
In girls, a foreign body can enter the uterus during masturbation or sitting on the ground without panties. It will provoke the appearance of purulent leucorrhoea.
In addition, the risk of getting foreign bodies into the uterus is that when this organ of the female reproductive system contracts, the spiral and so on can move into the abdominal region. As a consequence, the development of inflammation of the peritoneum. And this, in turn, is very dangerous.
The identification of unnecessary objects inside the uterus is facilitated, first of all, by ultrasound, and less often by radiography. Of course, a foreign body cannot but cause any symptoms, because sooner or later the foreign body must manifest itself.
The photograph shows the detection of foreign objects using ultrasound
The main features are:
- Change menstrual cycle, often spotting in the middle of the cycle. This means that the objects in the uterus have already oxidized and become covered with salts;
- Pain felt primarily in the vaginal area. They occur when the body is in the uterus for a long time;
- Purulent leucorrhoea.
Removing items
Most often, the removal of a foreign body occurs during the period when the corpus luteum matures in a woman’s body, that is, in the middle of the cycle. It is important to remove the excess as soon as possible and begin treating the inflammation before worms form inside.
After ultrasound examination or probing the uterus when it turns out that in female body if something unnecessary gets in, the gynecologist removes what is detected with a finger or using tweezers. If there is a narrowing of the entrance to the uterus, that is, stenosis, then the doctor will be able to remove objects only after opening the cervical canal.
It is worth noting the moment of pregnancy, when such a desired “foreign” object is attached to the wall of a woman’s uterus, with which she will live for the next nine months. However, the embryo does not immediately enter its cavity. This is preceded by the process when the corpus luteum is formed in the ovaries and ovulation, that is, fertilization itself. Some representatives of the fair sex completely mistakenly think that the corpus luteum, since it actively participates in the fertilization of the body, descends into the uterus. This is the deepest misconception - only in the ovaries. The corpus luteum of the menstrual cycle and pregnancy are divided. The second occurs after the birth of a new life - the formation of an embryo. It affects the functioning of the uterus, especially fallopian tubes, since the corpus luteum during pregnancy secretes much more progesterone than the corpus luteum of the menstrual cycle.
You can learn more about pregnancy by watching this video:
Thus, everything in a woman’s body is interconnected, and the so-called foreign substances that enter the body are also different.
This project was led by a 25-year-old woman. She has never given birth and has no history of STDs. Each photograph was taken at approximately 10:00 p.m., starting on the first day of the menstrual cycle. Throughout this project, she used condoms as a contraceptive method and also to prevent semen from being released during the photo shoot. She did not use tampons during her period.
This cycle is 33 days, which is the norm. The follicular phase of her cycle lasts until about 20–21 days. Favorable days for fertilization lasts several days from the 13th to the 21st day with ovulation on the 20th day. The luteal phase is 13 days (12–16 days is normal).
The above is for this cycle. As you can see, after ovulation on about the 20th day, her temperature began to rise due to increased progesterone, which in turn is produced by the corpus luteum. This temperature shift means that ovulation has already occurred.
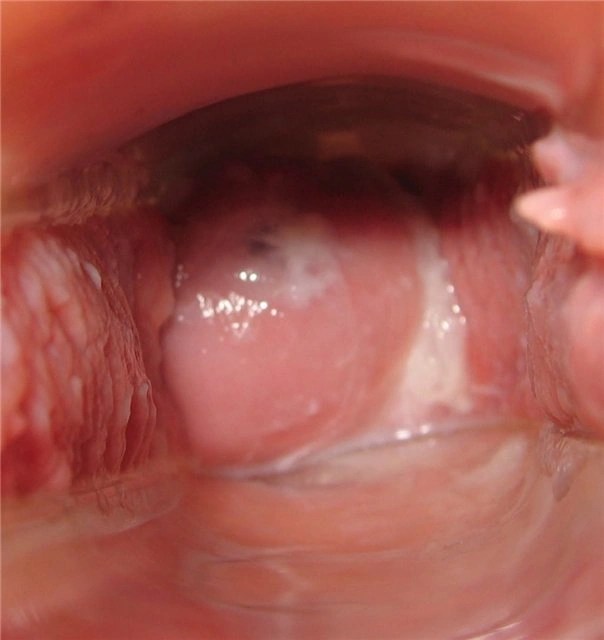
She also monitored the position of the cervix throughout the entire cycle. Since the photo does not show whether the cervix is hard or soft, high or low. All this is clearly noticeable upon independent palpation. The uterus is tilted back (retroflexion), you may notice in several photos that the cervix is pointing upward. These are anatomical changes that are present in 20–30% of women, and most often a genetic trait.

The first day
The blood is red, there are slight cramps in the lower abdomen.
Breasts are slightly swollen.
Feelings are very sexual.

Second day
The blood is dark red.
The breast is normal.

Day three
Blood is brown, sometimes watery dark red.

Day four
Note the fresh blood.

Day five
Brown color.
Tired state.

Day six
Very light brown discharge.

Day seven
The neck is in a low, closed position.
There is sticky liquid on the neck.
Day eight
The neck is low and closed.
Cervical fluid is white and sticky.

Day nine
The neck is low and closed.
Feeling dry.

Day ten
The neck is low and closed.
Note the drop of blood and brown lump near the cervix (right). Perhaps from a stormy conversation on the same day, but later an endometrial polyp was diagnosed.

Day eleven
Cervical fluid is creamy.

Day twelve
Cervical fluid is white milky. Feeling wet.
I feel especially sexy.

Day thirteen
Copious watery discharge.
The neck is softened and moves upward.

Day fourteen
White, transparent, watery cervical fluid that stains underwear.

Day fifteen
The cervical fluid changes to a discharge that resembles egg white.
The neck is soft, open and high.

Day sixteen
Cervical fluid in the form of egg whites, very wet.
The neck is soft and high.


Day seventeen
Cervical fluid is very thin, with whitish-yellow streaks. Sensual breasts, but not painful.
The liquid stretches between the fingers when stretched.

Day eighteen
Egg white.

Day nineteen
Egg white with a white tint.

Day twentieth
Minor back pain and cramps on the left side.
Suspicion of ovulation.
Feeling of strong sexuality.
Cervical fluid like gelatinous egg white.

Twenty first day
Cervical fluid is like glue.
The nipples are very sensitive and painful.

Day twenty two
Painful nipples.
The neck is in the middle position and slightly open.
Basal body temperature begins to rise.

Day twenty-three
Very sensitive nipples.
Feeling dry.

Day twenty-four
Very sensitive nipples.
Dry.
The neck is firm and high.

Day twenty five
Headache and fatigue.
Cervical fluid is dry/sticky.

Day twenty six
Breasts are swollen.
Basal body temperature is now noticeably higher, by about 1 degree.

Day twenty seven
Painful nipples, swollen breasts.
Cervical fluid is sticky.

Day twenty eight
Feeling dry.

Day twenty nine
Feeling dry.

Day thirty
Feeling dry.
The chest is heavy.

Day thirty one
Feeling bloated.
Dry, (note, fresh blood, a sign of impending menstruation).
Feeling emotional instability.

Day thirty two
Light brown spots.
The neck is low and open.
Feeling tired.

Day thirty three
Pink spots.
Pain in the lower back.
Menstruation will begin tomorrow after waking up, 13 days after ovulation.
The article was taken from the internet! For those who are not interested, don’t fu... fuck!
– the presence of a foreign object in the cavity or wall of the uterus, accompanied by a complex of pathological disorders. Foreign bodies of the uterus can manifest themselves as bleeding, chronic endometritis, pyometra, pain syndrome, and secondary infertility. Foreign bodies of the uterus are detected using ultrasound, hysteroscopy, and probing. Removal of foreign bodies of the uterus can be performed during hysteroscopy, curettage of the uterine cavity, laparoscopy; in complicated cases, hysterectomy may be required.

General information
In the uterine cavity, the presence of loose or ingrown intrauterine contraceptives and their parts (threads, plastic hangers, metal fragments), surgical ligatures, and fetal bone fragments is often detected. Sometimes foreign bodies that enter the uterus are encapsulated and do not manifest themselves for a long time. In other cases, foreign bodies may move with muscle contraction, cause perforation of the uterine wall and migrate into the uterus. abdominal cavity or retroperitoneal space. Infection of foreign bodies of the uterus causes a chronically ongoing inflammatory process that is not amenable to active therapy. The problem of detection and removal of uterine foreign bodies in clinical gynecology is relevant due to the likelihood of developing a wide range of dangerous complications.
Symptoms of a foreign body of the uterus
Clinically, uterine foreign bodies usually manifest themselves as changes in menstrual function - menorrhagia, metrorrhagia, spotting. If foreign bodies remain in the uterus for a long time, they cause chronic endometritis, secondary infertility, and sometimes the development of pyometra. The presence of IUD fragments may be asymptomatic.
Appearance pain syndrome, as a rule, indicates perforation of the uterine wall by parts of the IUD and can lead to further migration of objects and injuries to neighboring organs. Perforation of the uterus can be partial (the IUD is inserted into the myometrium) or complete (the IUD completely or to some extent extends beyond the uterine wall). When foreign bodies migrate from the uterus, they can be found in the area of the omentum, rectosigmoid angle, Bladder, appendicular process, uterine appendages, retroperitoneal space, in the cecum or small intestine.
Bone remains of the fetus are most often accidentally discovered in patients examined for prolonged endometritis, menstrual irregularities, and secondary infertility. The history of this category of women reveals termination of pregnancy at 13-14 weeks or more, usually complicated by bleeding and repeated curettage of the uterine cavity. Lavsan or silk ligatures are usually detected in patients with endometritis, pyometra, or previous obstetric or gynecological interventions (caesarean section, conservative myomectomy, etc.). In this regard, patients are concerned about purulent leucorrhoea and secondary infertility.
Diagnosis of a foreign body in the uterine cavity
The main method for detecting a foreign body of the uterus, which gynecology has today, is hysteroscopy. Other instrumental studies (chair examination, probing, ultrasound, laparoscopy) have auxiliary meaning. During a gynecological examination, a foreign body in the uterus can be detected using a probe. The disadvantage of probing the uterine cavity is the impossibility of determining the exact location of the object, its nature, shape and size, and its relationship to the walls of the uterus and neighboring organs.
Conducting a transvaginal or transabdominal ultrasound is more informative for detecting intrauterine contraceptives. Fragments of the IUD in the form of zones of increased echogenicity can be found directly in the uterine cavity or in the thickness of the myometrium. Ultrasound diagnosis of bone remains and ligatures in the uterine cavity is difficult and uninformative.
The hysteroscopic picture depends on the nature of the uterine foreign body. Foreign bodies remaining in the uterus for a long time can become covered with endometrium, intrauterine synechiae, salts, and also form bedsores in the wall of the uterus. With the help of hysteroscopy, it is possible to determine the location of a foreign body of the uterus and carry out its targeted removal. Bacteriological examination of the smear allows you to select adequate antibiotic therapy based on the sensitivity of the microflora to the drug. Foreign bodies lying loosely in the abdominal cavity are detected by plain radiography.
Removal of a foreign body from the uterus
Foreign objects lying in the uterine cavity can be specifically removed through the hysterocope canal using endoscopic instruments. It is not recommended to remove uterine foreign bodies blindly, since such attempts can lead to fragmentation and deformation of foreign objects, as well as injury to the uterine wall. If partial or complete perforation of the uterine wall is detected, hysteroscopy is combined with laparoscopy.
In the case of foreign bodies growing into the thickness of the endometrium, curettage of the uterine cavity with removal of the detected fragments is indicated. Sometimes colpohysterotomy, a transvaginal incision of the uterus, is used to remove foreign bodies. In situations where foreign bodies extend beyond the uterus, penetrate into neighboring organs or the abdominal cavity, a laparotomy is performed with revision of the organs concerned.
If the presence of a foreign body in the uterus is complicated by perforation and massive infection, removal of the uterus may be necessary: supravaginal amputation or hysterectomy. In the postoperative period, antimicrobial treatment is carried out. Prevention of the presence of foreign bodies in the uterus involves careful monitoring of the condition of the uterine cavity after removal of the IUD, abortion, and gynecological operations.
Instead of an introduction
“If youth knew, if old age could”(proverb)
- You see, yesterday I left the operating room in good mood“, a gynecologist surgeon I know told me, “the operation was not complicated, but delicate. All that was needed was nothing: to remove the overgrown part of the fallopian tube, and transplant the healthy remainder of it into the corner of the uterus.
At that not so distant time, there was not yet “ high technology type IVF” and the opportunity to make happy a woman exhausted by infertility with overgrown openings of the fallopian tubes, gynecologists associated with the plastic restoration of their patency.
– The operation was successful, I think that patency will be restored and, perhaps, the patient will fall into the 70% pregnancy rate that PVM (Chief’s initials) had.
Today's problem surgical treatment tubal infertility has “gone” into the background. But there was a time when leading clinic specialists “competed” to achieve the best results.
- And so, in this good mood, I go into the staff room and what do you think? I see the Calendar Year there! Twelve employees gathered for a short lunch break. In terms of faces, characters, length of service, and experience, this is like your 12 months. On the tables between the case reports are tea cups, homemade sandwiches and other lunch items. And everyone is talking animatedly about something at the same time. January, February, March glanced sideways at the creaking of the door. To my short “Salute!” They looked around in surprise and continued the serious conversation, not understanding my mood. Taking the operation log, he sat down on the sofa and, concentrating, began to describe the operation performed. Naturally, I involuntarily listen to the peaceful conversation, and oh God! What do you think they were talking about? About bras. For a moment it seemed that I was not in a 140-bed clinic, but in a store women's clothing. The hand trembled and began to unsteadily trace the progress of the operation. Ugh - you! Tried to change the course of a business discussion by loudly asking: who read last number magazine "Obstetrics and Gynecology"? April, May, June turned around and, sipping tea, looked at me as if I were empty space. July asked: “What’s interesting there?” August, combative and fast, retorted: “You need to read Solomatin!” September, October, November stood up and, finishing their chewing, said: “Homo sapiens, you better come down to us, to the delivery room, there you will see everything that is written in your journal.” And even December, the 72-year-old Doctor - Veteran, who was sitting by the window and correcting the mistakes of all Eleven in the medical histories, raised her head, silently looked around everyone and again went deeper into her work, which made it possible to submit medical documentation without delays. statistics.
“By the way,” he asked, “have you read Solomatin?”
“No, I haven’t read it,” I answered, “but what?”
“They say he writes interestingly, and everything about our brother, obstetricians and gynecologists.”
Intrigued, I looked on the Internet. And there... “Tatyana Solomatina is a candidate medical sciences, former obstetrician-gynecologist..." And a list of books.
I’m holding in my hands “Obstetrician-Ha!” Evil, but in a good way. He makes jokes, but there are also sober thoughts. From the review of journalist Yu. Vasilyev: “ Thanks to this book, you will take a new look at familiar things: doctors and patients, illness and recovery, the problem of fathers and children, life and death...”
The chapter “First Night” begins with the words: “Getting a medical specialty is not so easy.” Reasonable and... exciting. The chapter ends: “ P. S. And the doctor, in addition to attentiveness and non-disgust, materialism and superstition, faith and disbelief, participation in the mysteries of life and death, is characterized by the speed of reactions, like fighter pilots or special forces officers for capturing secret military points deep behind enemy lines.”
That's it, and you're talking about bras.
I turn the page, the next chapter is “Glory to Russia.” It turns out that this is addressed to glassblowers. A short story, only 2 pages, but it got me thinking.
The essence of the story is a humorous presentation of a very serious gynecological issue about foreign bodies. The patient complained of urinary disorder. Upon questioning, it turned out that two or three years ago she was recommended to measure the temperature in the vagina. I inserted the thermometer and fell asleep. When I woke up, I didn’t find a thermometer. There were no disorders. She became pregnant, gave birth, and was healthy. And now, several years later, doctors cannot establish the cause of dysuric disorders. Thanks to the ultrasound, they identified a foreign body in the bladder. It turned out that an ordinary, completely intact glass mercury thermometer, which suddenly disappeared three years ago, was lying in the bladder. A funny episode, but it makes me sad.
From memories
“All stupid things on earth are done with a smart face”(Baron Munchausen)
Episode 1. As a 6th year student, our subordinates, the leading teacher, associate professor Nikolai Viktorovich Andrezen, took us to the educational museum of the department when covering the topic “Abortion”. This museum was founded in the clinic in the second half of the 19th century by Professor K.F. Slavyansky and was constantly replenished. In it, among numerous macropreparations, he showed us a “set” of objects extracted from the genital tract of women who got there in various ways, most often through criminal abortions.
The picture is impressive (Fig. 1).
Fig. 1 A set of objects removed from the genital tract.
On the recommendation of the associate professor, I go to the library, open M.G. Serdyukov’s book “Forensic Gynecology and Forensic Obstetrics” and on page 291 I read: “ It goes without saying that presence in the genitals during pregnancy or abortion of various foreign bodies" (pieces of bougie and rubber tubes, plant roots, pieces wood, fragments of a crochet hook, remnants of fabric or rope, and in one rare case, for the purpose of abortion, a woman giving birth inserted a medical thermometer into her uterus) serves as an indication of an abortion.”
And he gives two examples. A Hegar dilator No. 5 was removed from one of the abdominal cavity, which got there during a criminal abortion performed six months ago. In another, “... a twig from a broom, wrapped in gauze, 19 cm long and 10 cm thick different parts 0.5-0.3 cm(p.292).
Several years later, he acquired his own experience in removing a foreign body from the uterus.
Episode 2. While already in graduate school, he worked part-time on weekends and holidays in the so-called “septic gynecological department.” One day, as usual on Sunday, at 9 o'clock I went on duty. The morning was calm, there were no emergency patients. I made a leisurely “introductory” round, talked with the patients and, having finished, settled down in the resident’s room with my dissertation affairs. After a while, one of the women in the department comes in and shyly says that she wants to tell you something. He invited me to sit down. I took the medical history and found out that she had been in the hospital for two days. She was admitted on Friday with a diagnosis of febrile spontaneous threatening abortion during 10 weeks of pregnancy. There is no bleeding, and the temperature is high up to 38 o -39 o, so we observed him while carrying out antibacterial therapy.
- Tell me.
“Upon admission, I was embarrassed to talk about the intervention for the purpose of abortion.
“What kind of intervention is this?” I asked her, who turned out to be a nurse at one of the hospitals.
– Doctor, this is not my first abortion. I always challenged him by inserting a hair pin. She took it by the ends and inserted it into the cervix with the blunt end. And everything was fine. And this time the pin slipped into the uterus.
“Here’s grandma and St. George’s day,” I thought. The calm morning quickly ended. As the hero of the movie “Liquidation” said: “Oil painting.” The algorithm of action, as they say today, was clearly outlined in my head: X-ray→ clarification of the diagnosis → further decision.
I called “03”, explained the situation, asked for help, and 5 minutes later I received an answer: a traumatology department on duty with an X-ray machine on the other side of the city. Well, it's a long day. I ask for understanding and help. They sent a “transport”, took it, did it, brought it back with a photo. Here it is, right in the palm of your hand, lying across the uterine cavity: the curved part to the right, the tips to the left.
Then it's a matter of technology. Under local infiltration anesthesia with a 0.25% solution of novocaine, paracervically, 120 ml, dilation of the cervical canal to No. 12, careful entry into the uterus with a long Kocher forceps, groping, grasping and leisurely removal of the pin (Fig. 2). Then excochleatio ovi and abrasio cawi uteri. A day later, the patient was discharged in satisfactory condition.
Fig.2.
 When I reported this clinical observation at a meeting of the Kazan Society of Obstetricians and Gynecologists, Mark Iosifovich Slepov, associate professor at GIDUV, spoke in the debate and said:
When I reported this clinical observation at a meeting of the Kazan Society of Obstetricians and Gynecologists, Mark Iosifovich Slepov, associate professor at GIDUV, spoke in the debate and said:
-You were lucky, there was a metal object. But I suffered in a similar situation, removing a glass eye rod from the uterus. All I could think about was how not to crush it into fragments. But everything turned out well.
Or it may not be possible and you will have to resort to surgical intervention. In the museum of the department there is exhibit No. 114, which is a fragment of the tip of a Brown syringe (Fig. 3). The accompanying inscription says that Dr. V.V. On March 24, 1923, Dyakonov had to cut the cervix to the internal os and only then was it possible to remove the foreign body from the uterus.
Fig.3. Brown syringe tip fragment
 The moderator of the meeting, Professor Pavel Vasilievich Manenkov, recommended to “look” at the “Course of Obstetrics and Women’s Diseases” by prof. V.S. Gruzdeva. The boss's recommendations must be followed.
The moderator of the meeting, Professor Pavel Vasilievich Manenkov, recommended to “look” at the “Course of Obstetrics and Women’s Diseases” by prof. V.S. Gruzdeva. The boss's recommendations must be followed.
I open the first part of “Anatomy and Physiology of the Female Reproductive Apparatus” (M., 1919) and on page 14 I read: “...the female urethra differs from the male urethra in its length, the width of the lumen and especially its extensibility: length it is only from 3 to 4 centimeter, and the extensibility is so significant that the urethral canal can be easily stretched with bougies to a diameter of 1 cm and even so much that it can be inserted into the bladder forefinger».
Today, against the background of existing methods for examining the bladder, examination of its walls through the dilated urethra is completely forgotten. There was a reason for this special set Simon's mirrors. This is what V.F. wrote about this. Snegirev (Uterine bleeding. M., 1895, 2nd edition, p. 34): “...star-shaped shallow cuts are made on the external urethra, penetrating through the mucous membrane and muscle tissue and gradually begin to insert mirrors from a smaller number to a larger one. Already at No. 6, the urethra is so dilated that one can easily pass the index finger through it, and at No. 7, at artificial lighting easy to readper visumwith the color of the mucous membrane of the bladder or neoplasm in it.”
I open the second part “Obstetrics” (Berlin, 1922, volume 2) and on page 209 I read: “Insertion of bougies, etc. into the uterus. objects is the favorite method resorted to by “specialists” and “specialists” in criminal miscarriages... in villages for this purpose they use tools such as spindles... In my practice there was a case where a peasant woman, trying to insert a spindle into the uterus, pierced her in several placesseptum vesico— vaginal, causing the formation of several vesicovaginal fistulas; However, she was unable to terminate the pregnancy; subsequently she was safely delivered of the pregnancy at full term, and a few months later I sewed up all her fistulas.”
I open the third part “Gynecology” (Kazan, 1922) and on pp. 90-91 in the section on diagnostic methods I read that “ X-ray studies could be successfully used in gynecological practice... to recognize metallic foreign bodies in tissues and organs" in cases where “...correct diagnosis is extremely difficult due to the reluctance of patients, out of a sense of shame, to reveal to the doctor the true cause of the disease. I myself once had to remove from a young girl’s bladder, through a previously dilated urethra, a head pin, which was strongly curved and caused unbearable suffering to the patient (Fig. No. 64). Undoubtedly, the patient herself inserted the hairpin there while masturbating; however, she stubbornly continued to deny this both before the operation and after the pin was removed.”
We recognize the hairpin from “Gynecology” by Prof. V.S. Gruzdev in the “set” of foreign bodies from the museum in Fig. No. 1. Well, how? Have you arrived?
And further. In the section “Traumatic injuries of the female genital organs” (pp. 195-203), Prof. V.S. Gruzdev devoted three pages to injuries associated with foreign bodies. He's writing: “A relatively common source of traumatic injuries to the genital apparatus in women are the so-called. “foreign bodies”, most often found in the sleeve, less often in the uterus, bladder, parts of the abdominal cavity adjacent to the genital area, etc.... The purposes for which they are introduced are varied... These bodies themselves are extremely diverse... various instruments , pessaries (often homemade), hysterophores, bougies, head pins, knitting needles, corks, balls of thread, wooden balls, wine glasses, fondant jars, coils, candlestick heads, cow horns, etc., etc.” (Gynecology. Kazan, 1922, 1st edition, p. 199).
And further (NB!). “Remaining in the genital canal, bladder or abdominal cavity, sometimes for years, even decades, foreign bodies can ultimately have a strong irritating effect on the walls of the vagina, bladder, etc., can then penetrate into the thickness of these walls and, finally, , perforate them. Moreover, on this basis fistulas can arise - vaginal-vesical, vaginal-rectal, etc. "(ibid.).
An example of “creativity and diversity” is exhibit No. 95, stored in the department’s museum. This is a piece of dry reed (Fig. 4).
Fig.4.
 Judging by the explanatory text, “the grandmother’s instrument for causing a miscarriage” was delivered to the museum of the department by Dr. V.S. Kandaratsky, who, while working as an emergency doctor, in 1926-1928 was a freelance resident with prof. V.S. Gruzdeva.
Judging by the explanatory text, “the grandmother’s instrument for causing a miscarriage” was delivered to the museum of the department by Dr. V.S. Kandaratsky, who, while working as an emergency doctor, in 1926-1928 was a freelance resident with prof. V.S. Gruzdeva.
And we find a completely “exotic” description of criminal abortion from another student of Prof. V.S. Gruzdev - resident I.V. Danilov (future professor, head of department, director of GIDUV). That's the essence of it. A 24-year-old woman’s “grandmother” injected a goose feather into her uterus to terminate a pregnancy of approximately 3 months. The insertion “... lasted a long time and was painful.” She tied the outer end of the feather with a harsh thread to her right thigh. The woman was at home for three days. There was no miscarriage. On the 4th day, she went to the hospital due to chills and severe bleeding from the genital tract. Having examined it, Ivan Vasilyevich did not find the feather, and the thread went into cervical canal. It was not possible to remove the feather by pulling it, but per rectum was found in the posterior Douglas “... solid, in the form of a stick, as thick as a finger.” By curettage of the uterine cavity, he removed the fertilized egg and at the same time identified a perforation hole on the posterior wall of the uterus. Emergency transection. A goose feather 9.5 cm long and a thread 70 cm long were removed. Damage internal organs did not have. The hole in the uterus is sutured. Recovery (Kazan medical journal, 1931, pp. 907-908). For more details, see our methodological manual“Perforation of the uterus” (Kazan, KSMU, 2000).
By the way, in connection with the issue under discussion, we strongly recommend reading the book by L.E. Ulitskaya - “The Case of Kukotsky” (M., 2004).
Episode 3. Once a young woman, virgo, came in with complaints of foul-smelling vaginal discharge, which appeared, in her words, “out of the blue.” During the examination, we were lucky: the hymen turned out to be easily stretchable and the hole in it freely allowed the index finger to pass through. I palpate some soft formation that resembles cotton wool. Using a long Kocher clamp, I carefully grab the lower pole and pull it out freely with a slight pull. Bah! Yes, this is a swollen sanitary tampon. The patient was embarrassed and remembered that she had used it not so long ago, but believed that she had removed everything in a timely manner. The procedure was completed by washing the vagina with a weak solution of potassium permanganate followed by administration of a dose of olazole.
Surgery greeted the end of the 19th and beginning of the 20th centuries with the introduction and development of asepsis and antisepsis. In Kazan, prof. V.S. Gruzdev following prof. N.N. Fenomenov actively used surgical methods for treating gynecological patients. In this regard, a new problem has arisen: foreign bodies left in the abdominal cavity during surgery.
Joke. In the old days, the professor finished the abdominal operation, changed his clothes and was anxiously looking for something, holding the bridge of his nose.
Operating nurse - What did you lose, professor?
Professor - Pince-nez. I can't remember where it might be?
Operating nurse (jokingly) - In the patient’s abdominal cavity, professor.
Professor - Really? Urgent x-ray! This is true.
Prepare relaparatomy.
A joke is a joke, but the matter is very serious these days.
Throughout the twentieth century, publications about such incidents periodically appeared, and even now appear. So recently, a popular publication reported that one lady, during security control at the airport, discovered a metal object that had been forgotten in the abdominal cavity during an operation performed several years ago.
Prof. V.S. Gruzdev drew attention to this problem at the very beginning of his activity with the publication of the article “On the issue of foreign bodies in the abdominal cavity and the relationship of the peritoneum to them” (Russian Doctor, 1906, No. 30, p. 917), soon reprinted on German. A few years later, in his “Course,” he returned to this issue in the section on injuries to the female genital organs: “ Among the foreign bodies in the abdominal cavity that a gynecologist has to deal with, the majority are instruments, gauze compresses, etc. objects introduced here during abdominal transections and then forgotten here...
I myself once had to remove a clamp through the vaginaTerrier, at 22 s. long (Fig. 150), forgotten in the abdominal cavity after ovariotomy... the instrument remained in the abdominal cavity for 7 years... Upon examination, I was convinced that in the patient’s stomach there was, clamped, a long instrument, the top of which, having perforated the abdominal wall, protruded sant. 2 above its surface, the handle can be felt in the posterior vaginal fornix. I was able to remove this instrument by posterior colpotomy relatively easily, and 2 weeks after that the patient was completely healthy"(Gynecology. Kazan, 1922, 1st edition, p. 199). The removed clamp has been kept in the department museum for more than 100 years as visual material(Fig. 5).
Rice. 5.
 This question worried him all his life and he drew public attention to it for the third time in the publication “On the issue of the responsibility of gynecologists and surgeons for leaving instruments and other objects in the abdominal cavity of patients during abdominal operations” (Kazan Medical Journal, 1926, no. 2, p.215).
This question worried him all his life and he drew public attention to it for the third time in the publication “On the issue of the responsibility of gynecologists and surgeons for leaving instruments and other objects in the abdominal cavity of patients during abdominal operations” (Kazan Medical Journal, 1926, no. 2, p.215).
We also observed a similar incident.
Episode 4.
“No, life is not only a May day,
Where everyone dances and sings..."
(from song)
In 1989, in December, in Kazan, on the initiative of the Ministry of Health of the TASSR, KSMI, RKB and the Scientific Society of Therapists, a republican scientific and practical conference was held on the problem “Medical errors: causes, ways to overcome.” “Theses” of reports were published (Kazan, 1989). In the fifth section “Obstetrics and Gynecology”, the curious Reader will find our publication “Timely diagnosis of foreign bodies in the abdominal cavity during cesarean section” (pp. 156-159). It outlines the circumstances and medical tactics in two observations. That's their essence.
Observation 1. A 34-year-old pregnant woman has an emergency caesarean section. A boy weighing 3200 g was removed under general endotracheal anesthesia. During suturing of surgical wounds of the uterus and abdominal wall, the anesthesiologist asked to speed up the operation due to the lack of narcotic drugs necessary to continue anesthesia, because it was nearing the end of duty. After applying skin sutures, the surgeons, due to the haste that arose, suspected that they had left napkins in the abdominal cavity, placed in it for isolation before removing the fetus. The operating nurse confirmed the surgeons’ fears, but unfortunately, after suturing the abdominal wall. To confirm, an urgent ultrasound was performed: “there is a homogeneous shadow in the lateral parts of the abdomen.” They resorted to urgent laparoscopy - gauze pads were found located behind the uterus; extracted. Postoperative period without complications.
Observation 2. A 32-year-old woman in labor underwent a cesarean section during her third term labor due to persistent weakness of labor. In the postoperative period, intestinal paresis occurred for 9 days. Treatment was carried out with varying success. The suspicion of leaving a foreign body was categorically rejected by the operating doctor. Laparoscopically on the 9th day the presence of such was revealed. Relaparotomy. A diaper was removed and inserted into the abdominal cavity to isolate it before removing the fetus. The doctor present at the relaparotomy, who performed the caesarean section and was confident of complete sinlessness, fainted. Prolonged postoperative period, discharged on the 21st day.
The conclusions are as old as eternity: to prevent the abandonment of a foreign body during transection, there must be maximum mobilization of the attention of the surgeon, his assistants and the operating nurse. At the slightest suspicion, immediate clarification of the diagnosis is necessary. Neglect of this leads to severe complications, delayed removal of the foreign body and a protracted postoperative period.
Episode 5. I'll tell you about one more case from personal experience. Once I had to operate on a patient I knew with a large cystic tumor, the upper border of which was at the level of the navel. For safety and greater confidence, I asked Associate Professor I.F. to assist. Polyakova. After opening the abdominal cavity, it was determined that it was a giant parovarian cyst (a macroscopic specimen is kept in the museum of the department). Its enucleation was associated with the exposure of an extensive interligamentary surface, on which there were multiple pinpoint bleeding areas. There was no electrocoagulator. I used small gauze pads, taking several pieces in my hand at a time and pressing them onto the bleeding areas. Ivan Filippovich reminded me several times that such small tampons need to be taken with clamps, because... you can lose them in the abdominal cavity. I deliberately violated this attitude. Large gauze napkin folded specific situation It was inconvenient to use, and one swab on the clip was not enough. Accepting the assistant’s comments, he asked him to increase his vigilance. He himself tried to hold these tampons in his fingers as tightly as possible. Before suturing the abdominal wall, we carefully examine the abdominal cavity. And what do you think? One after another, three (!) small gauze swabs were found, lying loosely in different parts of the abdominal cavity. I think comments are unnecessary. At that moment I was put to shame and looked with gratitude at my wonderful friend and assistant, Associate Professor Ivan Filippovich Polyakov, silently looking at me. There is no point in talking about further experiences. The postoperative period passed without complications. I breathed a sigh of relief only after the patient was discharged home. The woman lived for a long time and, already at an advanced age, died from a severe extragenital disease. I am grateful to my colleagues. The secret of negligence was delicately kept. Although they say that the winner is not judged, however, it is impossible to escape self-condemnation. Self-flagellation is not the best thing. Today this secret was revealed for the first time for you, Dear Reader. Judge if you want, have mercy if you want.
Episode 6. We have already talked above about the possible long-term, years-long presence of a foreign body of the uterus in the abdominal cavity. The outcomes are very varied. Several such observations took place in the clinic of prof. V.S. Gruzdeva.
Observation 1. The woman was admitted with a diagnosis of recurrent ovarian tumor. From the anamnesis it was established that about two years ago she was operated on at her place of residence for an ovarian cyst. The postoperative period was complicated by infiltration at the site of the removed tumor. The therapeutic measures taken “significantly reduced the size of the infiltrate.” Throughout the year I felt satisfactory, but recently I began to feel nagging pain in the right iliac region. She contacted a gynecologist, who discovered a fixed tumor-like formation in the area of the right appendages and referred the patient to Kazan. The examination revealed that to the right and slightly behind the uterus there is a round, with clear contours, slightly painful, dense, immobile tumor, reminiscent of ovarian fibroid. Ablation. Extensive adhesive process, which made tumor removal difficult. The latter measures 12x15 cm. On the section: a dense, thick, up to 1 cm pseudocapsule; there is a gauze napkin in the cavity. Recovery. The macroscopic specimen is preserved in the museum of the department (Fig. 6)
Rice. 6.
 When this observation was reported at a meeting of the scientific society of obstetricians and gynecologists, prof. N.E. Sidorov shared his experience of removing a gauze pad from the bladder in the debate. It was forgotten in the abdominal cavity during the operation to remove the tumor. Over time, a bedsore formed in the wall of the bladder, and a napkin found during cystoscopy penetrated there.
When this observation was reported at a meeting of the scientific society of obstetricians and gynecologists, prof. N.E. Sidorov shared his experience of removing a gauze pad from the bladder in the debate. It was forgotten in the abdominal cavity during the operation to remove the tumor. Over time, a bedsore formed in the wall of the bladder, and a napkin found during cystoscopy penetrated there.
And also, about forgotten napkins from the story of Associate Professor V.I. Zhuravleva:
A year after caesarean section A woman with suspected foreign bodies in the abdominal cavity was taken to the gynecological department of the Republican Clinical Hospital of the Ministry of Health of the Republic of Tajikistan at her place of residence. During the examination, clearly visible protrusions of the anterior abdominal wall were found in the epigastric region, symmetrically from the midline close to the costal arches. Upon palpation, they give the impression of the presence of infiltrates, and ultrasound revealed foreign bodies. A surgeon was invited - associate professor V.V. Fedorov. A collective decision was made to undergo surgical treatment. Since the infiltrates were intimately connected to the anterior abdominal wall, we limited ourselves to dissecting the abdominal wall above them without entering the abdominal cavity. Two 20x20 cm napkins were removed. Further anti-inflammatory treatment. The outcome is recovery.
Observation 2. The woman was admitted 8 months after surgery for an ectopic pregnancy, complicated by postoperative infiltration in the posterior pouch of Douglas. Community treatment remained without effect. At that time I was mastering treatment inflammatory processes and they put her in my room. During the examination, there was indeed an infiltrate of “woody” density behind the uterus, moderately painful, without clear boundaries, approximately 7x8 cm in size. During puncture through the posterior fornix, there was a sensation of “entering the cartilaginous tissue.” No content received. Anti-inflammatory therapy was carried out for a week. Naturally without success. After a week of observation, Prof. P.V. Manenkov recommended repeat puncture with a larger diameter needle. Frankly speaking, I doubted the need for such, since there was not only fluctuation, but not even a hint of any softening of the infiltrate. However, the assignment must be fulfilled. The operating nurse prepared a syringe with a thick needle, which I inserted into the infiltrate as deep as possible. Pulling the plunger and at the same time slowly removing the needle, I completed the procedure. The syringe is empty. But what is it? Is there some kind of thread at the tip of the needle? Truly, “there would be no happiness, but misfortune would help.” I carefully inspect and find a barely noticeable notch on the tip of the needle, which caught and pulled out a thread from the depths of the infiltrate. And then “like a bolt from the blue” it dawned on me: a napkin! Then it’s a matter of technique: colpotomy, removal of a 20x20 cm napkin, anti-inflammatory therapy, recovery. The patient was discharged with recommendations to continue rehabilitation in the local resort of Bakirovo.
Observation 3. And also, in connection with ectopic pregnancy. The woman was admitted two months after surgery with infiltration in the stump. During the examination, I found a dense infiltrate to the left and behind the uterus without clear contours, dense, 6x7 cm, slightly painful. Prof. During his rounds, P.V. Manenkov, having carefully weighed all the circumstances of the case and especially the fact that the woman had been continuously receiving anti-inflammatory therapy at her place of residence for two months without any effect, recommended transection due to a suspicion of a foreign body. They entrusted me to carry it out. The abdominal cavity was opened. I carefully separate the adhesions and find nothing but “cartilaginous density.” Pavel Vasilyevich stood nearby and gave advice. My hesitant actions brought him out of patience and he, taking a long probe, began to poke it into different areas. And in one place it suddenly fell deep into the infiltration. There turned out to be a cavity of 1.5x2 cm, in which lay two silk ligatures and a small amount of cloudy liquid, which turned out to be an emergency laboratory research sterile. Sanitation. Suturing. Recovery.
"Not there"
We have already quoted above the statement of Prof. V.S. Gruzdeva about the great distensibility of the female urethra. Here's another one: " I have had occasion to observe more than once married women with a congenital absence of a sleeve, who apparently had sexual intercourse through the dilated urethra without any special disorders" (“Course of obstetrics and g.b.” M., 1919, part I, p. 14).
Anyone who has been more or less interested in congenital absence of the vagina or colpopoiesis is familiar with the work of prof. B.V. Sherstneva on colpoelongation. With the help of the device he invented, he was able to obtain sufficient deepening of the tissues of the vestibule of the vagina and the adjacent area due to their extensibility and thereby create conditions for coitus. A similar situation can arise in natural conditions. So in Kazan honey. and. (1926, vol. 2, pp. 209-210) an article by L.N. Sobolev “The case of a 16-year-old sexual life in the absence of a vagina and uterus.” Word to the author. " The patient got married at the age of 21. Firstcoitusthere was no pain and blood and, apparently, it was not successful... this went on for 2-3 years. Gradually, however, sexual intercourse became more normal...coitusbrought both complete satisfaction... this patient has vaginal aplasia... and under the influence of sexual activity the back partfossae navicularisand front wallrectumstretched, retracted into the rectum and formed a kind of vagina, quite suitable forcoitus ′ A».
She went to the doctor only because she had no children. In this situation, the reason for an infertile marriage is easily explained.
In the practice of an obstetrician-gynecologist, there are even more “exotic” observations that explain a woman’s infertility.
Episode 7. Once, a woman close to our family, embarrassed, asked to help her establish the cause of infertility. We have been married for more than a year, but pregnancy has not occurred. I asked for a consultation with Prof. P.V. Manenkov. He always responded willingly to the requests of young employees. There was only one condition: it was necessary to first try to understand the diagnosis ourselves, and then invite him for a consultation. This time, to his short answer: “Did you watch it yourself?”, I answered negatively, citing deontology. A friend, they say it’s inconvenient and something else like that. After carefully questioning the patient, he began the examination. At some stage, he suddenly asked me to step away to the side and began quietly asking the woman about something. I didn’t hear their conversation, but it was noticeable that the patient was overly worried. Having completed, as they say in the textbook, the additional anamnesis, he performed a rectal-abdominal examination and, briefly saying “everything is fine,” released the patient. He asked me to come into his office. Sitting down in a chair, he said:
–Your friends have a variant of dyspareunia.
I heard this term for the first time. Then, after rummaging through the reference book, I found that “Dyspareunia is the general name for sexual disorders in women. Consists of “dys” (Greek) - prefixes mean “difficulty”, “deviation from the norm”, “dysfunction”. And “pareunos” (Greek) – sleeping with someone in the same bed, cohabitant (Encyclopedic Dictionary of Medical Terms. M., 1982, vol. I, p. 356).
– Your friend virgo. Coitus takes place between the partner's closed thighs. I explained everything to her in detail. Don't forget to report the result.
“When the princess retired with him,
You could tell that the night didn't last long.
Filled with abundant dew -
A pink bud opened in the night,
Rain flowed drop by drop into the pearl oyster
And the pearl was born in the shell.
The darkness of the night has not yet thinned,
This peri carried her in her womb.”
And it all ended the same way, according to Ferdowsi:
“The circle of forty weeks has ended,
Like the sun, the princess’s son was born.”
When I reported to the professor about Andryushka’s birth, he only smiled with satisfaction and mysteriously.
This is how we went through Gruzdev’s school, marveling at the wisdom and delicacy of the Teacher.
P.S. When we meet, students always ask to tell us something they remember from their more than half a century of work as an obstetrician-gynecologist. What is presented in this essay is only a small part of what I experienced. Oddly enough, the cases most often remembered are not from obstetrics and gynecology, but from general medical practice: one case of saving 6 year old girl from diphtheria croup, and the second - restoration of hearing in a 70-year-old grandmother. Both are associated with the ENT specialty.
But more about that next time.
L.A. Kozlov, Doctor of Medical Sciences, Professor
Department of Obstetrics and Gynecology No. 1 KSMU
(Head of the department - Prof. Khasanov A.A.)







